
AMA (WA) COVID EMERGENCE PLAN
THE SAFEST WAY FORWARD
EXECUTIVE SUMMARY

- The slow and steady entry of COVID-19 into Western Australia is optimal to allow systems to be tested and measures put in place as well as minimise risk of the health system being overrun.
- WA should adopt a VACCINE PLUS approach to living with COVID:
- VACCINE – the best method to reduce death and disease; and
- PLUS – all other measures to reduce transmission, such as personal hygiene, environmental, systems and protocols.
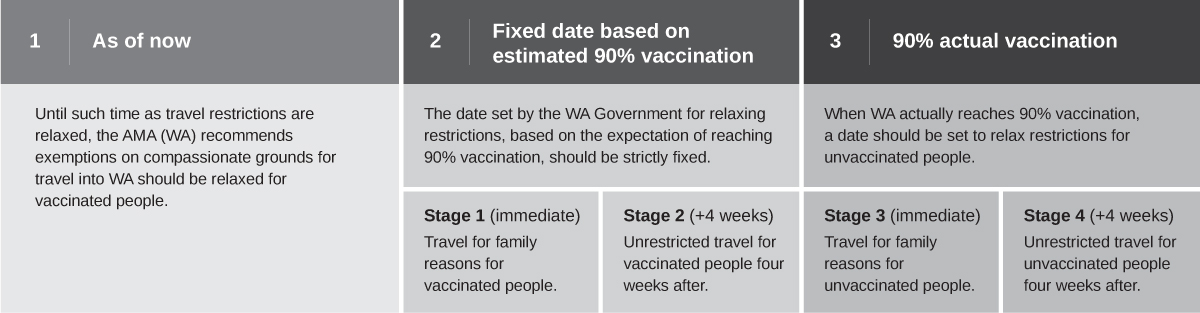
- A more compassionate border should be enacted now for fully vaccinated individuals with appropriate pre-travel testing, testing on arrival, and while in quarantine.
- Given the leaky history of our hotel quarantine system, home quarantine should be considered for fully vaccinated travellers, with testing at appropriate intervals.
- Fully vaccinated residents should enjoy freedoms earlier than those unvaccinated, to encourage vaccination, protect the unvaccinated and reduce the rate of viral spread in the community.
- Relaxed travel restrictions should be staged.
- Active preparation for living with COVID should happen now, including for hospitals, GPs, schools, regional towns and aged care facilities.
MODELLING
 Evidence-based modelling, real-life experience in other states (NSW and Victoria), and level of preparedness should be the basis for WA’s plan for COVID emergence.
Evidence-based modelling, real-life experience in other states (NSW and Victoria), and level of preparedness should be the basis for WA’s plan for COVID emergence.- The AMA (WA) agrees with the State Government’s target threshold of a 90 per cent double-dose rate (of eligible persons) before reducing travel restrictions.
- ANU/UWA modelling suggests that we should strive for 90 per cent of the total population to avoid significant disease and death. WA hospitals are currently not in a position to manage a COVID outbreak unless 90 per cent of the population is double vaccinated.
- The UK’s National Health Service (NHS) reports long COVID rates of 7.4 per cent in the paediatric population aged 2-11.
SETTING A DATE
- The AMA (WA) supports setting a date to relax restrictions for fully vaccinated people, to encourage vaccination.
- The WA Government has the most up-to-date information on modelling data and should be the body that sets dates.
- The date should also be based on evidence of adequacy of hazard controls and preparation.
- Reduced travel restrictions should be staged.
- We do not support a travel date being set for unvaccinated people until WA reaches a 90 per cent vaccination rate.
- In setting a date, the Government should consider the medical workforce – 350 new doctors, who are due to start work in January 2022, will require 2-4 weeks to be inducted, educated, fit tested and trained in PPE.
- We agree with the WA Government’s established safeguards for arrivals, including:
- Negative PCR result within 72 hours of departure;
- Testing on arrival and in quarantine;
- If quarantine is required, preferably to be at home; and
- Arrangements to be set by government.
- However, we recommend that relaxed travel restrictions should be staged to minimise the risk of overwhelming our hospitals. The staged approach should be as follows:
VACCINE PASSPORT FOR DOMESTIC WA ACTIVITY

We agree with the WA Government that proof of vaccination (‘vaccine passports’) should be applied for access to social events with COVID-spread risk, such as large-capacity events as well as pubs and clubs.
The use of vaccine passports should be initiated prior to the introduction of relaxed restrictions to enhance preparation and improve vaccination rates.
HEALTH SYSTEM PREPAREDNESS
PUBLIC HOSPITALS
- Preparation should continue with clinician-led plans.
- Clinical reference groups should include members from all medical specialties.
- All hospitals should have a plan on how to reduce staff infection – attention should be given to all levels of controls to prevent outbreaks from staff transmission with:
- Safe indoor air ventilation
- CO2 monitoring
- HEPA filters as required
- Fitted N95 and elastomeric PPE
- Administrative and testing controls.
- The WA Government should consider that approximately 350 new doctors will be starting work in January 2022 and will require 2-4 weeks to settle in with induction, education, fit testing and PPE training.
- Rapid Antigen Testing (RAT) when and where appropriate.
- Protocols for patient screening in tertiary hospitals and elective surgery should be developed now.
SUPPORTING GPs and PRIVATE SPECIALISTS

- GPs and private specialists should be supported to make improvements to all levels of hazard control to prevent and manage outbreaks in their practices, including safe indoor air ventilation, fitted N95 masking and administrative controls.
- GPs may well be able to manage the home care of patients unwell with COVID, with the comprehensive development of protocols and controls, which is preferable to placing stress on the ambulance and emergency medical access systems.
- RAT should only be used when appropriate in 2022 (i.e. when evidence shows that RAT will be most effective, for example, when there is a higher prevalence of COVID).
- Protocols for patient screening in tertiary hospitals and elective surgery should be developed now.
- A community monitoring (vitals and oxygen saturation) and treatment model must be developed with exhaustive GP engagement. Relevant organisations to be consulted include the AMA (WA), WA Primary Health Alliance (WAPHA) and the Royal Australian College of General Practitioners (RACGP).
- Appointments of unvaccinated patients should be accommodated at a specific time of day to minimise interaction with vaccinated patients and allow more appropriate system exposure controls for staff.
- There must be a plan for escalation of care for the deteriorating patient.
REGIONAL AREAS
 The WA Government should consider providing additional medical and nursing support to rural hospitals, which are already understaffed and are therefore vulnerable to being overwhelmed in the event of an outbreak – remembering that only Bunbury Regional Hospital has an ICU.
The WA Government should consider providing additional medical and nursing support to rural hospitals, which are already understaffed and are therefore vulnerable to being overwhelmed in the event of an outbreak – remembering that only Bunbury Regional Hospital has an ICU.- There must be a plan for escalation of care and transfer of critically ill and ventilated patients from the country.
- If the plan is for patients to be treated in regional areas rather than being transferred to metropolitan hospitals, they face a higher risk of death. Country patients should therefore be advised of this risk to allow planning, lobbying and more informed decision-making regarding vaccination.
CONCERN FOR VULNERABLE GROUPS
ABORIGINAL COMMUNITIES
 Aboriginal communities should be supported, with well-resourced and funded plans in place for their particular circumstances.
Aboriginal communities should be supported, with well-resourced and funded plans in place for their particular circumstances.- The WA Government should utilise expertise from Aboriginal health organisations, trusted Elders and the wider Aboriginal community.
- The approach of people having ‘had a chance, and refused’ is not appropriate. Rather, the reasons for refusal should be explored and managed in a culturally respectful way.
PREPARATION OF SCHOOLS
- WA Schools should actively be preparing for endemic COVID disease now. In October 2021, 320 schools were closed across NSW and Victoria due to COVID outbreaks.
- If the schools are closed, kids are missing out on the school environment, classes and social interaction.
- The AMA (WA) supports a VACCINATION PLUS Program for schools. This includes:
- Maximisation of school age vaccination rates. Pfizer is now being given to 5 to 11 year olds with FDA and advisory panel (ATAGI equivalent) approval.
- In Australia, TGA and ATAGI approval is expected in early 2022 and the first two weeks of school in February could be used for a school-based vaccination program if approved. The timing of that approval and practical application of a vaccination program for the 5 to 11-year-olds should be a consideration in reducing restrictions given the 7.4 per cent long COVID rates reported in children by the NHS.
- Maximising natural ventilation
- Servicing air-conditioning units to ensure optimal airflows
- Use of HEPA filters
- Use of masks if there is an outbreak
- Use of CO2 monitoring to check ventilation
- Outdoor classes where safe
- Minimise mixing of class groups at breaks.
- Rapid Antigen Testing (RAT) when and where appropriate.
- Protocols for screening of students should be developed now.
MENTAL HEALTH PATIENTS
- Any planning needs to consider inpatient and community psychiatric patients.
- Use of a mobile clinic/bus to visit hostels/clinics should be considered
AGED CARE FACILITIES
Preparation should start now, including:
- Maximising natural ventilation
- Servicing air-conditioning units to ensure optimal airflow
- Use of HEPA filters
- Use of masks if there is an outbreak
- Use of CO2 monitoring to check ventilation
- Rapid Antigen Testing (RAT) when and where appropriate
- Protocols for screening should be developed now
PUBLIC EDUCATION
- The WA Government needs to continue to strongly promote and support ongoing vaccinations, including boosters.
- Organisations and businesses need to be supported to continue providing indoor safe air controls, masking and SafeWA app use to assist contact tracing.
- WA citizens should understand that we are likely to move from a society with minimal restrictions to having more restrictions in the short-term. Increasing the ability for people to travel will coincide with social restrictions such as mask-wearing on public transport, and at large events.
POLITICS-FREE
- The safe reduction in travel restrictions for WA should be based on the safety and welfare of Western Australians and in no way should be used as a political tool to influence the Federal Election.
REFERENCES
Doherty Modelling Report for National Cabinet 30 July 2021. Accessed 9 Nov 2021
Hyde Z et al. High vaccination coverage is required before public health measures can be relaxed and Australia’s international border fully reopened. Version 14 Aug 2021
NHS 2021 NHS sets up specialist young people’s services in £100 million long COVID care expansion 15 June 2021 Accessed 9 Nov 2021
Guardian 2021. Accessed 17-11-2021